Class XI Biology: Breathing and Exchange of Gases
This chapter covers the mechanics of how we pull oxygen from the atmosphere and push it into our bloodstream, while simultaneously scrubbing out the toxic CO2.
The Breath of Life: Mastering Breathing and Exchange of Gases
Respiration is more than just “inhaling and exhaling.” It is a multi-step transport system. The goal? To get Oxygen to the mitochondria of your cells so they can produce ATP, and to remove Carbon Dioxide before it turns your blood acidic.
In this chapter, we explore the Respiratory Volumes of the lungs, the “magic” of Hemoglobin, and the physics of Partial Pressure that allows gases to move without using any energy.
The Core Pillars of Respiratory Physiology
1. The Respiratory Interface
Humans have a highly branched network of tubes ending in Alveoli. The alveoli are the primary sites of exchange. They are incredibly thin—composed of a one-cell thick epithelium—to allow for rapid diffusion across the respiratory membrane.
Getty Images
2. The Mechanism of Breathing
Breathing is a game of pressure gradients.
- Inspiration: The Diaphragm and External Intercostal muscles contract, increasing thoracic volume and lowering intra-pulmonary pressure. Air rushes in.
- Expiration: Muscles relax, thoracic volume decreases, and pressure rises above atmospheric levels. Air rushes out.
3. Transport of Gases
- Oxygen: 97% is carried by Hemoglobin (as Oxyhemoglobin).
- Carbon Dioxide: 70% is carried as Bicarbonate ions, 23% by Hemoglobin, and 7% dissolved in plasma.
The Gauntlet: 10 Challenging Aptitude Questions
Question 1: The Alveolar Barrier
The diffusion membrane is made of three layers. Name them and explain why the total thickness is much less than a millimeter.
Question 2: Pulmonary Volumes
Match the following respiratory volumes with their average values in a healthy adult male:
- Tidal Volume (TV): ?
- Inspiratory Reserve Volume (IRV): ?
- Expiratory Reserve Volume (ERV): ?
- Residual Volume (RV): ?
Question 3: Vital Capacity Calculation
If a person has a Tidal Volume of 500 mL, an IRV of 2500 mL, and an ERV of 1100 mL, what is their Vital Capacity (VC)?
Question 4: Partial Pressure Gradient
At the alveolar site, what is the pO2 (Partial Pressure of Oxygen) and pCO2 (Partial Pressure of Carbon Dioxide)? How does this compare to the pressures in deoxygenated blood?
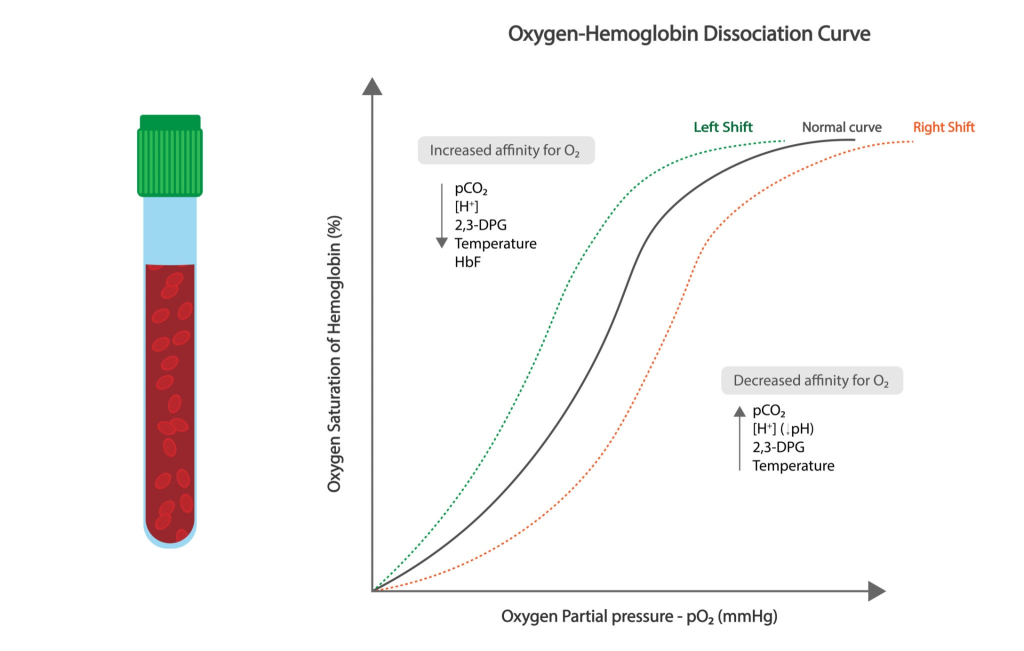
Question 5: The “Sigmoid” Curve
The Oxygen-Hemoglobin dissociation curve is sigmoid-shaped. What factors cause this curve to shift to the Right (decreasing the affinity of Hemoglobin for Oxygen)?
Question 6: The Carbonic Anhydrase Engine
Which enzyme, found in high concentrations in RBCs, facilitates the conversion of CO2 and H2O into Bicarbonate (HCO3–)?
Question 7: The Bohr Effect vs. Haldane Effect
Briefly explain the difference between the Bohr Effect (how CO2 affects O2 binding) and the Haldane Effect (how O2 affects CO2 binding).
Question 8: Respiratory Center
Where is the Pneumotaxic Center located in the brain, and what is its primary role in regulating the duration of inspiration?
Question 9: Occupational Hazards
Identify the respiratory disorder caused by long-term exposure to stone-breaking or grinding dust, leading to Fibrosis of the upper lung tissues.
Question 10: The Emphysema Paradox
In smokers, the alveolar walls are damaged, and the surface area for gas exchange is significantly reduced. What is this chronic disorder called, and why is it irreversible?
Detailed Explanations & Solutions
1. Alveolar Barrier
The three layers are: 1. Thin squamous epithelium of alveoli, 2. Endothelium of alveolar capillaries, 3. Basement substance between them.
Result: Its extreme thinness (approx. 0.5 micrometers) ensures that gases can diffuse in milliseconds.
2. Pulmonary Volumes
- TV: 500 mL
- IRV: 2500–3000 mL
- ERV: 1000–1100 mL
- RV: 1100–1200 mL
- Result: Residual Volume is the air that stays in the lungs even after the most forceful expiration.
3. Vital Capacity
VC = TV + IRV + ERV.
Result: 500 + 2500 + 1100 = 4100 mL.
4. Partial Pressure Gradient
- In Alveoli: pO2 = 104 mmHg; pCO2 = 40 mmHg.
- In Deoxygenated Blood: pO2 = 40 mmHg; pCO2 = 45 mmHg.
- Result: Oxygen flows from Alveoli (104) to Blood (40), while CO2 moves from Blood (45) to Alveoli (40).
5. Curve Shift (Right)
A shift to the right means Oxygen is “unloaded” more easily.
Result: This is caused by High pCO2, High H+ concentration (Low pH), High Temperature, and high 2,3-BPG.
6. Carbonic Anhydrase
Result: This enzyme is found in cytoplasm of RBCs and allows CO2 to be transported safely as Bicarbonate in the plasma.
7. Bohr vs. Haldane
- Bohr Effect: High CO2/Low pH causes Hb to release O2 (at tissue level).
- Haldane Effect: High O2 binding causes Hb to release CO2 (at lung level).
- Result: They work together to ensure efficient gas exchange at both ends of the circuit.
8. Respiratory Center
Result: Located in the Pons region of the brainstem. It acts as a “switch-off” point for inspiration, thereby limiting the duration of breath and increasing the rate.
9. Occupational Hazards
Result: Silicosis and Asbestosis. Prolonged exposure leads to the proliferation of fibrous tissues (Fibrosis), causing serious lung damage.
10. Emphysema
Result: Emphysema. Cigarette smoke destroys the elastic alveolar walls, merging tiny alveoli into large “sacs.” This reduces the surface area for exchange permanently.
Pro-Tip: The “CO2 Solubility” Fact
CO2 is 20–25 times more soluble than O2. This is why CO2 can diffuse across the respiratory membrane just as effectively as Oxygen, even though its pressure gradient (only 5 mmHg) is much smaller than Oxygen’s gradient (64 mmHg).
")


